Overview of Main Reflexes affecting development
The Fear Paralysis reflex
The Fear Paralysis reflex (FPR) is the first withdrawal reflex to develop in utero shortly after conception. It is a shutdown response by the embryo, whereby it withdraws and freezes in response to a threat to it or the mother. It is expected to be inhibited with the emergence of the Moro reflex in utero and should therefore not be present at birth.
When it is retained beyond birth, it manifests as an overactive withdrawal response to sensory or psychological stimuli. Its persistence can also result in difficulties with attachment and difficulty accepting or giving affection easily. Social and emotional security will also be affected.
A child with an unintegrated FPR may withdraw both mentally and physically into their own internal safer space from new or unknown experiences, such as a parent departing, a birthday party, etc. Consequently, they are not engaging with and learning from these events which impedes development of their social skills and their ability to self regulate.
School-aged children may try to pass under the radar. They may be perfectionist and experience a strong fear of failure. Such children may face chronic anxiety and fears and struggle with panic disorders.
Often an unintegrated Fear Paralysis withdrawal response will coexist with the fight / flight Moro, the next in the developmental sequence of reflexes.
Behaviors that may be observed in a child with a retained Fear Paralysis reflex :
Low tolerance to stress
- Excessive shyness
- Constant feelings of overwhelm/anxiety
- Withdrawal from social situations
- Difficulty making eye contact
- Hypersensitivity to sensory stimuli
- Poor adaptability and flexibility and reluctance to engage in new activities
- Compulsive traits and phobias
- Lack of confidence and low self-esteem
- Over/under attachment to adults and peers
- Selective mutism
- Separation anxiety
- Sleep challenge
The Moro reflex
The Moro reflex emerges in utero 9 to 12 weeks following conception. It is normally fully developed at birth and inhibited in its crude form and transformed into the adult startle response at around 4 months. In utero, the Moro helps develop the breathing mechanism and provides the energy and adrenaline to start the birthing process. It can be triggered to facilitate the first breath of life if breathing has not started naturally. The Moro reflex consists of a sudden symmetrical movement of the arms up and away from the body with the hands open. This is accompanied by a sharp intake of breath and then a gradual folding in with the return of the arms across the chest into a clasping posture, pulling up of the legs and may be followed by a cry. It is the earliest sympathetic nervous system adrenalised fight/ flight response and acts as a survival mechanism in the first months of life, signalling to the outside world that the baby is in difficulty and needs attention.
The Moro has multi-sensory triggers and can be activated by any of the senses including auditory with a loud or unexpected noise, visual with an unexpected change in light levels or movement in the visual field, tactile with intense touch, pain or a sudden change in temperature, vestibular with an alteration in posture or balance.
When the Moro stays active, the ability to understand sensory stimuli is compromised and the fight/flight response is too easily triggered undermining the ability to differentiate between what is safe and not safe. The child will be in a state of reactivity and hypersensitivity and the excess release of stress hormones can impact the child’s physical and emotional well-being and affect behaviours.
The effects of a retained Moro are far reaching , but some possible symptoms of a retained Moro reflex include :
- Anxiety and fearfulness / angst (continuous anxiety seemingly unrelated to reality)
- Low self esteem and lack of confidence leading to insecurity /dependency or a need to control or manipulate events
- Emotional immaturity with a need for constant reassurance
- Dislike of change or surprise- poor adaptability
- Difficulty accepting and giving affection. Physical timidity
- Vestibular challenges such as poor balance and coordination
- Motion sickness
- Difficulty processing sensory information leading to distractability and hypersensitivity
- Weakened immune system leading to frequent ear, nose and throat infections and allergies.
- Immature eye movements and visual perception challenges
- Poor pupillary reaction to light, photosensitivity, difficulties with black print on white paper, dislike of fluorescent lights.
- Shifts between hyperactivity and extreme fatigue.
- Poor stamina
- Sleep challenges
The Palmar reflex / Babkin response
The Palmar grasp reflex develops in utero at about 11 weeks and is fully present at birth. It forms part of a group of reflexes whose common characteristic is to ‘grasp’. Pressure or touch to the palm of the hand will result in closure of the fingers with the thumb underneath. After several more weeks the response will include a gripping reflex in response to a pull against the finger tendons.
There is also a direct link between the Palmar and feeding in the early months with a Palmar being elicited by sucking movements and the action of sucking may trigger kneading movements in the hands. This hand /mouth link is called the Babkin response. If this neurological link persists we may witness tongue movements while carrying out activities involving the hands eg when colouring, writing or cutting with scissors.
The integration of the Palmar reflex marks the start of a journey to developing complex skills with the hands (voluntary holding and release of objects and independent thumb and finger opposition), allowing for development of fine motor skills, including controlling a pencil, doing up buttons etc.
Manual dexterity and manipulatory activities develop sensory and proprioceptive awareness of the hands. A weakness in coordination of the hands and fingers can result in tension in the wrists forearms and shoulders affecting writing posture.
Possible effects of a retained Palmar reflex / Babkin response:
- Poor manual dexterity due to challenges with independent thumb and finger movements, witnessed in difficulty with the ability to hold and use scissors, pencils and pens appropriately
- Immature pencil grip and consequent difficulty with handwriting
- Involuntary movements of the mouth/tongue when writing, drawing etc
- Speech difficulties due to the continued presence of the Babkin response which prevents the development of independent muscle control at the front of the mouth which will affect articulation.
Other grasping reflexes – Plantar and Babinski
Both of these reflexes develop in utero with the Plantar normally modulated during the first year of life and the Babinski by two years of age.
The Plantar is triggered by applying pressure or stroking the sole of the foot just under the toes. When the reflex is still active the toes curl and grasp.
The Babinski is elicited by stroking along the outer side of the foot causing the big toe to turn upwards, the toes to spread and the foot to invert.
Both of these reflexes prepare the toes and feet to play their crucial role of becoming upright.
Release of the plantar reflex allows the toes to lie in a flat position, providing stability when the child is upright and allowing coordination of a heel to toe stride.
The Babinski develops sensory awareness of the inside and outside edges of the feet, and helps develop the foot arches and ankle stability, which in turn supports the knees and hips.
Integration of both of the Plantar and Babinski help to give the child gravitational security, grounding them both physically and emotionally knowing where they are from the base.
Possible symptoms of retained Plantar/Babinski reflexes :
- Difficulties learning to walk
- Insecure balance (especially in the dark when vision cannot be used to compensate)
- Trips or falls over easily
- Very sensitive feet- ticklish
- Reduced running speed/ awkward running
- Immature foot arches and recurrent ankle weakness
- Toe walking
- Reduced eye/ foot coordination
Rooting and Sucking reflexes
The Sucking reflex develops first in utero and helps develop the mouth movements for suckling and feeding. It helps to strengthen the jaw and fine muscles and tongue movements eventually required for clear speech and articulation.
The Rooting reflex emerges a little later and is elicited when either side of the mouth is touched causing the head to turn to the stimulated side and the mouth to open as the infant ‘roots’ or searches for the nipple or teat. This reflex is strongest in the first few hours after birth and if it isn’t stimulated at the appropriate time, e.g. through scheduled feeding or ICU care it may be retained in a weakened form.
Both the rooting and sucking reflexes should ideally be integrated around four months after birth.
Modulation of the sucking reflex allows the tongue to move backwards to push food down with throat, as opposed to the upwards movement elicited by sucking.
Symptoms of retained Rooting /Sucking reflexes :
- Speech and articulation delays and difficulties (due to immaturity in the control of muscles of the lips, tongue and jaw)
- Difficulty with feeding, chewing and swallowing
- Continued desire for oral stimulation e.g. sucking of thumb, fingers or clothes
- Hypersensitivity to tactile stimulation on the face, lips and mouth
- Poor lip seal and possible dribbling
- Continued hand/mouth link (Babkin), giving rise to difficulty with independent movements of the hands / mouth
The Spinal Galant reflex
The Spinal Galant reflex emerges at 20 weeks in utero and remains active during the first 3 to 9 months of life during which time it is inhibited. The reflex is activated by tactile stimulation on either side of the spine and will result in distinct hip flexion on the stimulated side. This reflex is thought to assist in the birth process. During labour, contractions of the vaginal wall stimulate the reflex and the subsequent rotational movement of the hips in conjunction with head and shoulder movements elicited by the ATNR help the baby manoeuvre its way down the birth canal. A baby born by caesarean section will not receive this stimulation and the reflex may remain underdeveloped.
The reflex is important in establishing muscle tone in the lower back, isolation of movement of the pelvis and an awareness of the two sides of the torso.
If the Spinal Galant is retained on one side, the child may develop scoliosis of the spine. Children with a retained Spinal Galant may prefer to lie on the floor to watch TV or do homework, since sitting with their back against a chair may trigger the reflex.
Possible symptoms of a retained Spinal Galant reflex :
- Fidgeting and squirming -‘ants in the pants’, due to hypersensitivity to tactile stimulation. (hyperactivity)
- Dislike of tight waistbands and labels due to sensory sensitivity in the lower back area
- Poor bladder control and bed wetting beyond the age of 5
- Secondary issues with attention, concentration and short term memory
- Unbalanced. gait with impaired hip rotation and reduced coordination of upper/ body lower body
The Tonic Labyrinthine reflex (TLR)
The Tonic Labyrinthine Reflex has two separate patterns, TLR forwards and TLR backwards. The TLR forwards develops at 3 to 4 months in utero and is inhibited by about 4 months of life. Movement of the head forwards elicits bending of the arms and legs into the body (foetal position).
The TLR backwards emerges at birth and is gradually inhibited by approximately 3 years of age. Movement of the head backwards beyond the level of the spine will elicit extension in the neck, arms and legs.
The reflex forwards and backwards contributes to the development of muscle tone and correct head alignment necessary for good balance (vestibular functioning) and sense of self in space (proprioception). It helps develop symmetrical positioning of the limbs, the ability of the body to become upright and move with stability, balance and tone against gravity.
If not well integrated, movement of the head forwards or backwards will continue to control flexor /extensor tone and movement of the spine, arms and or legs, affecting balance and upright posture.
In addition, continued TLR activity will impede the development of the lifelong head righting reflexes. If head control is lacking, eye functioning will also be impaired, leading to visual instability and challenges with judging space, distance, depth and speed.
TLR in flexion
Possible symptoms of a retained TLR :
Generally :
- Insecure balance and reduced coordination
- Weak neck muscles
- Tendency to motion sickness/vertigo
- Walking up/down stairs is difficult and escalators may cause disorientation
- Difficulty judging distance, speed and spatial orientation (knowing where one is in space in relation to objects or other people).
- Visual alignment skills e.g. such as working with maths in columns may be impaired.
- Difficulty with spatial planning for drawing and writing including spaces between words and letter sequences, etc.
TLR Forwards :
- Hunched or stooped posture
- Poor sitting posture- may hold head in hands when sitting
- Hypotonicity- low muscle tone
- Child tires easily, frequently seeking to lean, sit or lie down (reduced stamina and endurance)
- Challenges in lifting the arms or climbing
- Fear of heights
TLR Backwards :
- Poor posture with a tendency to toe walk
- Hypertonicity- tight locked muscle tone
- Stiff jerky movements and lack of fluidity when walking/ running
The Asymetrical Tonic Neck Reflex (ATNR)
The ATNR usually emerges about 18 weeks in utero. Movement of the head to one side will elicits reflexive extension of the arm and leg on the side to which the head is turned and flexion of the opposite limbs. This reflex stimulates movement, developing muscle tone and stimulating the vestibular system (the balance mechanism) in utero. The ATNR assists the baby in the birthing process, helping the baby move down the birth canal and the reflex is also activated and reinforced during this passage. Sally Goddard explains that this may be one reason why children who are born by caesarean section are at higher risk of developmental delay.
After birth, the ATNR will help the baby, when lying on its tummy to free his nose and mouth for breathing by helping it turn its head to one side.
The ATNR helps to develop extensor tone and plays a key role in the development of early hand/eye coordination. As the arm extends on the side to which he baby’s head is turned and the baby sees and grasps objects , this encourages the baby’s visual field to extend to arms length and allows the baby to develop awareness of the arms being part of the body.
As the ATNR integrates, the potential for creating neurological connections between both hemispheres of the brain is established and this communication is essential for good auditory and visual processing and cooperative functioning between both hemispheres.
A retained ATNR is very disruptive to a child’s development, impairing fundamental processes of balance, hand eye coordination, eye tracking, binocular vision and bilateral movement giving rise to reading, writing and sporting difficulties. The vast majority of children with dyslexia have a retained ATNR.
Possible effects of a retained ATNR :
- Balance may be affected as a result of head movement causing changes in flexor /extensor tone on either side of the body.
- Homolateral instead of normal cross pattern movements when walking. Lack of fluidity/ rhythm.
- May sit awkwardly at the table, turning the body to one side when writing.
- Difficulty crossing the midline eg a right-handed child may find it increasingly hard to write on the left side of the page, creating a slope out from the margin or may turn the page to 90° and extend the arm of the writing hand to accommodate the reflex.
- Pencil grip may be tight to override the desire for the hand to open when the head is turned towards it.
- Poor expression of ideas on paper- discrepancy between verbal ability and academic performance.
- Difficulty learning to ride a bicycle or swim the crawl. as the child turns his head to breathe, the arm on that side will want to extend away from the body.
- Poor hand/eye , foot/eye coordination when catching or kicking a ball due to eye tracking issues and uncoordinated movement.
- Difficulty with horizontal tracking required for fluent accurate reading with the eyes frequently losing their place, particularly at the midline, causing omission of letters, words or even whole lines when reading (which may affect comprehension and will likely give rise to low reading stamina).
- Difficulty using two hands simultaneously in a coordinated way for handling cutlery, scissors for cutting etc
The Symmetrical Tonic Neck reflex (STNR)
This reflex emerges around 6-9 months after birth and should integrate at around 9 to 11 months. It is considered as a bridging or transitional reflex as it is short-lived, but participates in several important aspects of development.
The STNR is activated in two positions by movement of the head. When the baby’s head is flexed, the arms flex and the legs want to extend and when the head is in extension the muscles of the upper body extend and the legs flex. As the baby begins to gain stability, he starts to rock back and forth. Blythe suggests that when the STNR is active it may help in developing visual accommodation (shifting visual focus between near and far distance with movement of the head).
The rocking motion develops muscle tone and strength, especially in the hips and upper body and arms. As the STNR integrates, crawling on hands and knees becomes possible. It is through crawling that hand eye coordination is further developed as the baby’s eyes focus from one hand to the other across the midline. This skill will later be very necessary for being able to read without losing words at the midline and to be able to visually follow the moving hand when writing. It is through crawling that the sensory systems of balance, vision and proprioception connect and start to work in synchrony for the first time. Without this integration, balance, space and depth perception may be compromised.
The integration of the STNR is crucial to establish the ability to move the head without affecting muscle tone in the upper and lower sections of the body. Retained or residual STNR will affect sitting and standing posture and gait.
Possible effects of retained STNR :
- Infant may be late to crawl, omit crawling or revert to bunny hop movements, bottom shuffling or bear walking
- Poor sitting posture– slumped over desk when writing
- Child may wrap legs around chair or sit on legs to anchor them
- Child may often sit in W like position when sitting on the floor or prefer to lie on the floor when watching TV etc
- Difficulties with adjusting focus from near to far and vice versa giving rise to slow visual accommodation and therefore fatigue when copying from the board or have difficulty catching objects moving at speed, e.g. when playing ball sports
- Reduced hand / eye coordination for writing / drawing
- Possible hypotonus (weak muscle tone in upper body) giving rise to upper arm weakness- monkey bars, pushups and somersaults may be tricky
- Problems with coordination, attention and concentration can be secondary outcomes
- Difficulties swimming butterfly and breaststroke because of poor cooperation between lower and upper body
- Messy eating
The Postural Reflexes
Primitive reflexes lie at the base of the developmental pyramid, laying the foundations for all later functioning. The transition from primitive reflex responses to postural control is a gradual process. Postural reflexes are lifelong reflexes and should be fully established by 3.5 years of age. The postural reflexes can be categorized into two groups: the righting reflexes and the equilibrium reactions.
The ocular head-righting reflex (OHRR) and the labyrinthine head-righting reflex (LHRR) have the important role of maintaining head control in response to postural changes. The OHRR responds to visual cues whilst the LHRR responds to impulses from the vestibular system (balance mechanism) in the inner ear. They work in tandem to respond to information received, to enable the child to position the head appropriately in response to postural changes in order to maintain balance and stability. Stable head control is needed for the eyes to be able to operate optimally and stay fixed on a target in spite of movement of the body.
These head-righting reflexes along with other postural reflexes – the amphibian reflex and segmental rolling reflexes, allow the infant to develop head control, balance, and coordination, whilst rolling, crawling, standing, walking and eventually running.
Equilibrium reactions are elicited if balance is lost or if there’s a shift in the centre of gravity, e.g. the parachute reflex, where a child puts his arms out to reestablish balance or protect himself from a fall. Underdeveloped equilibrium reactions can make a child appear clumsy and poorly coordinated which may trigger negative comments from the peer group and difficulty with social integration.
Possible consequences of underdeveloped righting reflexes and equilibrium reactions:
- Difficulties with static and dynamic balance
- Poor posture and clumsiness
- Difficulty with gross and fine motor skills
- Lack of control of eye movements leading to difficulties with reading and writing
- Subsequent emotional/behavioral instability, which may instigate feelings of isolation
The Developmental Pyramid
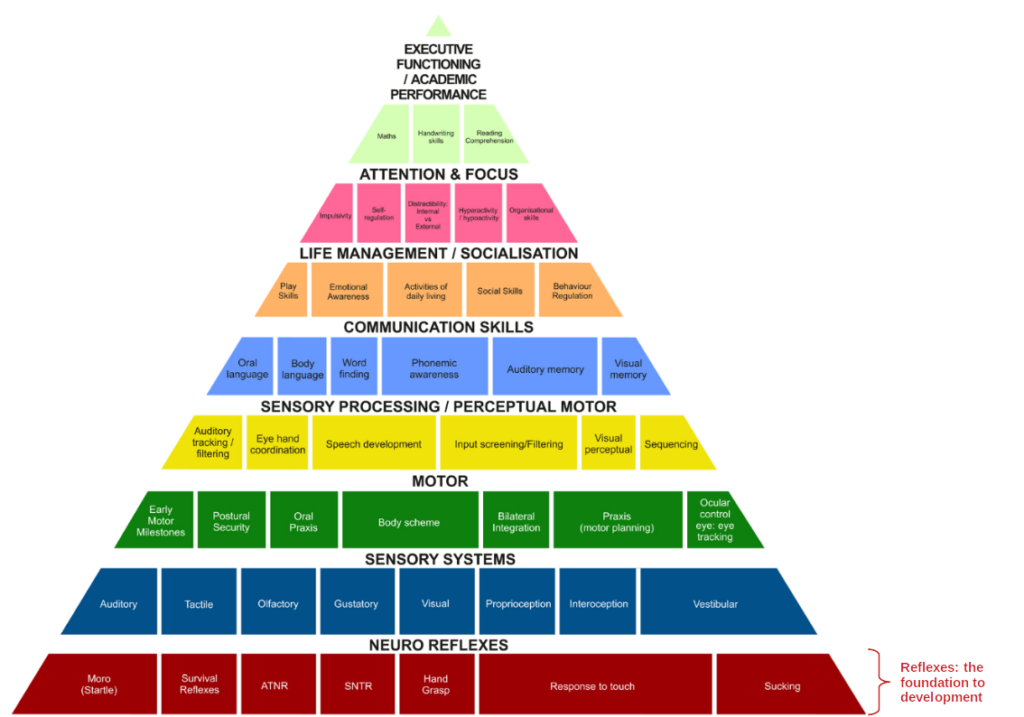
(Source : maximumpotential.org.uk)
CONTACT
Have any questions? I am always open to talk about your children and how I can help you.